Collaborators
David Moore
(Quick-Med Technologies)
William Toreki
(Quick-Med Technologies)
Roy Carr
(Quick-Med Technologies)
Bernd Liesenfeld
(Quick-Med Technologies)
Gregory Schultz
(Quick-Med Technologies, UF)
Albina Mikhaylova
(Quick-Med Technologies)
Paul Dominguez
(UF)
Jillian Vella
(Quick-Med Technologies)
Gerald Olderman
(Quick-Med Technologies)
Introduction
The primary vector of transmission for disease causing pathogens is hand contact. Even when rigorous protocols for hand washing and hygiene are followed, pathogens present on any contact surface can easily recolonize recently sanitized hands. Health care settings in particular increasingly demonstrate the problems of pathogen transmission leading to nosocomial infections due to the number of the highly susceptible populations in health care facilities. Other problems associated with regulatory pressures are also demonstrated by the fact that Medicare is planning to no longer reimburse for hospital-acquired infections– particularly MRSA.
“MRSA has become so common that in many hospitals more than half of all Staph infections tested are drug-resistant.”
– USA Today“The average hospital payment for a Pennsylvania patient who did not have an infection was $8,078, compared with $60,678 for patients who did.”
– Pennsylvania Health Care Cost Containment Council, Washington Post- USA Today reported in May 2006 that some hospitals are experiencing an increase of MRSA infections from 33% of all Staphylococcus aureus tested in 2000 to 75% in 2006.
- The CDC reports that nearly 4 per 1000 hospital discharges have acquired an MRSA infection, demonstrating a growing problem within the community from a community health perspective as well as a financial perspective.
- The Washington Post reports that a Pennsylvania hospital study indicated that 180 hospitals reporting nosocomial infections showed an additional billing of $2.3 billion of which only $614 million was collected from insurance.
A novel and useful improvement on existing hand sanitization technology is a leave-on skin sanitizer that continues to protect skin from bacterial colonization for hours after application. Continuing persistent protection of hands from colonization can interrupt pathogen transmission between caregiver and patient, between contaminated objects or surfaces and a person, and can prevent the contamination of a surface from a person that is not effectively sanitized. Quick-Med Technologies, Inc. (QMT) has developed an advanced “leave-on” skin sanitizer formulation by combining the immediate disinfection power of an alcohol-based product with the long-lasting antimicrobial persistence of an advanced bio-active polymer. Performance at the time of application matches that of common alcohol-based hand sanitizers; however, the NimbuDermTM advanced antimicrobial polymer formulation also provides continuous persistent efficacy against microbial contamination for a prolonged period against a wide range pathogenic bacteria associated with nosocomial infections including Staphylococcus aureus, Pseudomonas aeruginosa, as well as antibiotic-resistant organisms such as MRSA and VRE (up to 6 hours in laboratory testing, even after repeated rinsing with water).
The advanced NimbuDerm polymer is suitable for incorporation into various formulations and is compatible with common additives such as emollients (to help keep skin soft and hydrated), therapeutic nutrients, and other active ingredients. Antimicrobial skin care products formulated with NimbuDerm technology are the perfect choice for everyday use by both patients and health-care professionals seeking to reduce the spread of bacteria.
Benefits of NimbuDermTM Leave-On Skin Sanitizer
- Effectiveness-initial kill is greater than or equal to that of current alcohol based sanitizers on the market and is effective against a wide range of organisms including some viruses.
- Persistence-provides a bacterial barrier for at least 6 hours while easily removed with common soaps and water.
- Safety-NimbuDerm was found to fall within acceptable irritation levels per ISO 10993 method .
Problems with Currently Utilized Skin Sanitizers
- Solutions with alcohol as the active agent do not persist and can leave the sanitized skin both dry and flaky.
- Soap formulations with Triclosan as the active agent have shown high toxicity index ratings against infant dermal fibroblasts.
- Hydrogen peroxide solutions have shown a high toxicity index rating against keratinocytes.
- Povidone-Iodine solutions have been proven to show contact dermatitis in as little as 2% Iodine in solution in both allergy sensitive and non-allergy sensitive subjects and have been shown to inhibit human fibroblast growth.
 Fig. 1
Fig. 1 Fig. 2
Fig. 2Initial Effectiveness of NimbuDerm™ Skin Sanitizer
Figures 1 and 2. Left (A) and right (B) sections of agar plates display bacterial lawn of E. coli. Right (B) sections were inoculated with ~50 ul NimbuDerm, left sections (A) were left as negative controls, and the bottom sections (C) displayed the growth agar in its original state. The clear lack of growth on the NimbuDerm applied areas for both the EMB agar (left) and the WL nutrient agar (right) demonstrate both instantaneous kill and sustained microbicidal properties.
How NimbuDermTM Works
NimbuDerm utilizes polymeric quaternary polycationic microbicides and achieves its bacteriocidal activity by destabilization of the cell wall structures and by inducing cellular collapse without requiring entry of the antimicrobial agent into the cell itself.
NimbuDerm is unlikely to stimulate resistance in microbes based on their cell wall disruption mechanism and the ultimate large size of the molecule. Safety of these agents has been tested and was found to fall within acceptable irritation levels per ISO 10993 method.
 Fig. 3
Fig. 3Figure 3 (left). Section of pig skin partially treated with NimbuDerm (left half). The skin section was rinsed after treatment, then had Bromothymol blue indicator dye applied and was rinsed again. Blue area represents coverage of the treatment due to the electrostatic interactions between the dye and NimbuDerm.
NimbuDermTM Instant Effectiveness Versus a Leading Alcohol Based Hand Sanitizer
| Contact Time vs. P. aeruginosa (ATCC #15442) |
Average Log reduction, NimbuDerm |
Average Log reduction , Alcohol Based Sanitizer |
| ~1 second | 2.16 | 0.88 |
| ~15 seconds | 3.40 | 1.52 |
| 30 seconds | 5.25* | 2.24 |
| 1 minute | 5.25* | 2.20 |
| 3 minutes | 5.25* | 2.38 |
| 4 minutes | 5.25* | 4.43 |
| *indicates full kill Reference test methods 4, 5, and 6 |
||
Bactericidal Persistence Efficacy of NimbuDerm™ Skin Sanitizer Versus a Leading Alcohol Based Hand Sanitizer After 4 Hours
| Kill levels for: | % killed NimbuDerm | % killed alcohol based sanitizer |
|---|---|---|
| Staphylococcus aureus1,2 (ATCC #6538) | >99.9999% | <0.0% |
| Escherichia coli1,2 (ATCC #15597) | >99.9999% | <0.0% |
| Pseudomonas aeruginosa1,2 (ATCC #15442) | >99.9999% | <0.0% |
| Serratia marcescens1,2 (ATCC #13880) | >99.9999% | |
| MRSA2 (ATCC #BAA-44) | >99.9999% | |
| Vancomycin Resistant Enterococcus (VRE)2 (ATCC #700221) | >99.9999% | |
| Test method used was modified AOAC Use-Dilution Test (Reference 5) on 1glass slide and/or 2pig skin carriers at a 4 hour exposure – drying time for sanitizer ranged from 1 hour to 3 hours. | ||
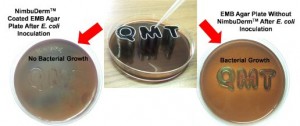
Figure 4 (above). Eosin Methylene Blue (EMB) agar plates inoculated with E. coli. The left plate had NimbuDerm applied before inoculation; the right plate has no treatment and serves as a control. Bacterial inoculum was applied into letterforms as shown on the center image, after NimbuDerm had dried on the plate. The EMB medium appears translucent green in response to E. coli metabolism. These images clearly demonstrate the ability of NimbuDerm to suppress bacterial growth on plates significantly after application of the skin sanitizer.
Antiviral Efficacy of NimbuDerm™ Skin Sanitizer
| NimbuDerm Drying Time: Contact Time with MS-2 Bacteriophage | Inativation efficacy |
|---|---|
| Drying time 0 minutes: 5 minute contact time | 99.93% Inactivation |
| Drying time 30 minutes: 5 minute contact time | 99.78% Inactivation |
| Drying time 4 hours: 5 minute contact time | 99.72% Inactivation |
| NimbuDerm Drying Time: Contact Time with Poliovirus | Inactivation efficacy |
|---|---|
| Drying time 4 minutes: 30 second contact time | 50.21% Inactivation |
| Drying time 4 minutes: 5 minute contact time | 68.40% Inactivation |
| NimbuDerm Drying Time: Contact Time with Herpes Virus | Inactivation efficacy |
|---|---|
| Drying time 30 minutes: 5 minute contact time | 99.78% Inactivation |
 Fig. 5 Cells before viral contact
Fig. 5 Cells before viral contact Fig. 6 Viral protection by NimbuDerm
Fig. 6 Viral protection by NimbuDerm Fig. 7 Viral infection without NimbuDerm
Fig. 7 Viral infection without NimbuDermVirus stock solutions {Bacteriophage MS-2(ATCC 15597B1), Poliovirus (strain Lsc1), and Herpes Simplex 1(HSV1)} were diluted to approximately 106 pfu/ml in Phosphate Buffered Saline (PBS). This viral dilution was used to evaluate the anti-viral efficacy of NimbuDerm by pipetting 100 μl of sanitizer into 24-well cell culture plates . At specified time points, 100 µl of the viral solutions was added to the well containing the NimbuDerm for specified contact times. Following the contact time, 2 ml of Difco Neutralizing Buffer was added to each well to neutralize the sanitizer and recover the virus. Dilutions of solutions containing the viruses were performed in PBS prior to enumeration. The number of viruses in each of the samples was enumerated as Plaque Forming Units (pfu) by an agar plaque assay. Plates were allowed to incubate overnight at 37°C and the plaques were then counted, and percent reductions as compared to the controls were determined.
Figure 5: Confluent monolayer of the Buffallo Green Monkey Cells (BGM) as positive control.
Figure 6: Undamaged cellular monolayer protected by the antiviral action of NimbuDermTM.
Figure 7: Plaque in BGM cell monolayer formed due to the Herpes virus infection.
Safety Testing
NimbuDermTM formulation has been tested for skin irritation and was found to fall within acceptable irritation levels per ISO 10993 method. Other materials from the NIMBUS technological family have been extensively tested for a full suite of ISO 10993 and FDA biocompatibility assessments, and were found to be non irritating (skin irritation and eye irritation testing), as well as non-sensitizing, and not eliciting any systemic toxic response. Guinea Pig Dermal Sensitization
Referenced Test Methods
- 1. ASTM E 1874-97, “Standard Test Method for Evaluation of Antibacterial Washes by Cup Scrub Technique.”
- 2. ASTM E 2315-03, “Standard Guide for Assessment of Antimicrobial Activity Using a Time-Kill Procedure.”
- 3. ASTM E 1053-97, “Standard Test Method for Efficacy of Virucidal Agents Intended for Inanimate Environmental Surfaces.”
- 4. ASTM 1153-03, “Standard Test Method for Efficacy of Sanitizers Recommended for Non-Food Contact Surfaces.”
- 5. AOAC, Use-Dilution Test, (955.14, 955.15, and 964.02).
- 6. AATCC 100-2004, “Antibacterial Finsihes on Textile Materials: Assessment of.”